Southern Africa has achieved clinical excellence in its HIV response. Even so, new infections continue to cluster predictably among adolescent girls, migrants, and marginalized communities, meaning the region’s HIV crisis is no longer primarily medical but structural. This article examines evidence from Soweto, Lesotho, and across the region to demonstrate how rigid health systems systematically fail populations whose lives are defined by mobility, economic precarity, and trauma. Epidemic control depends not on further clinical optimization, but on the political will to dismantle the structural inequalities, such as the legal frameworks, economic pressures, and inflexible service delivery that perpetuate disease transmission among the most vulnerable.
Southern Africa’s HIV response has achieved notable clinical success: viral suppression among those on treatment exceeds 90%, antiretroviral therapy is widely available, and treatment infrastructure rivals that of high-income countries. Yet the region still has approximately 21 million people living with HIV, and new infections persist among adolescent girls, migrants, and marginalized communities. This paradox shows that the crisis is no longer primarily medical but structural. The central problem is not a lack of treatment but a misalignment between rigid health systems and the precarious realities of vulnerable populations—mobility, economic instability, trauma, and social exclusion.
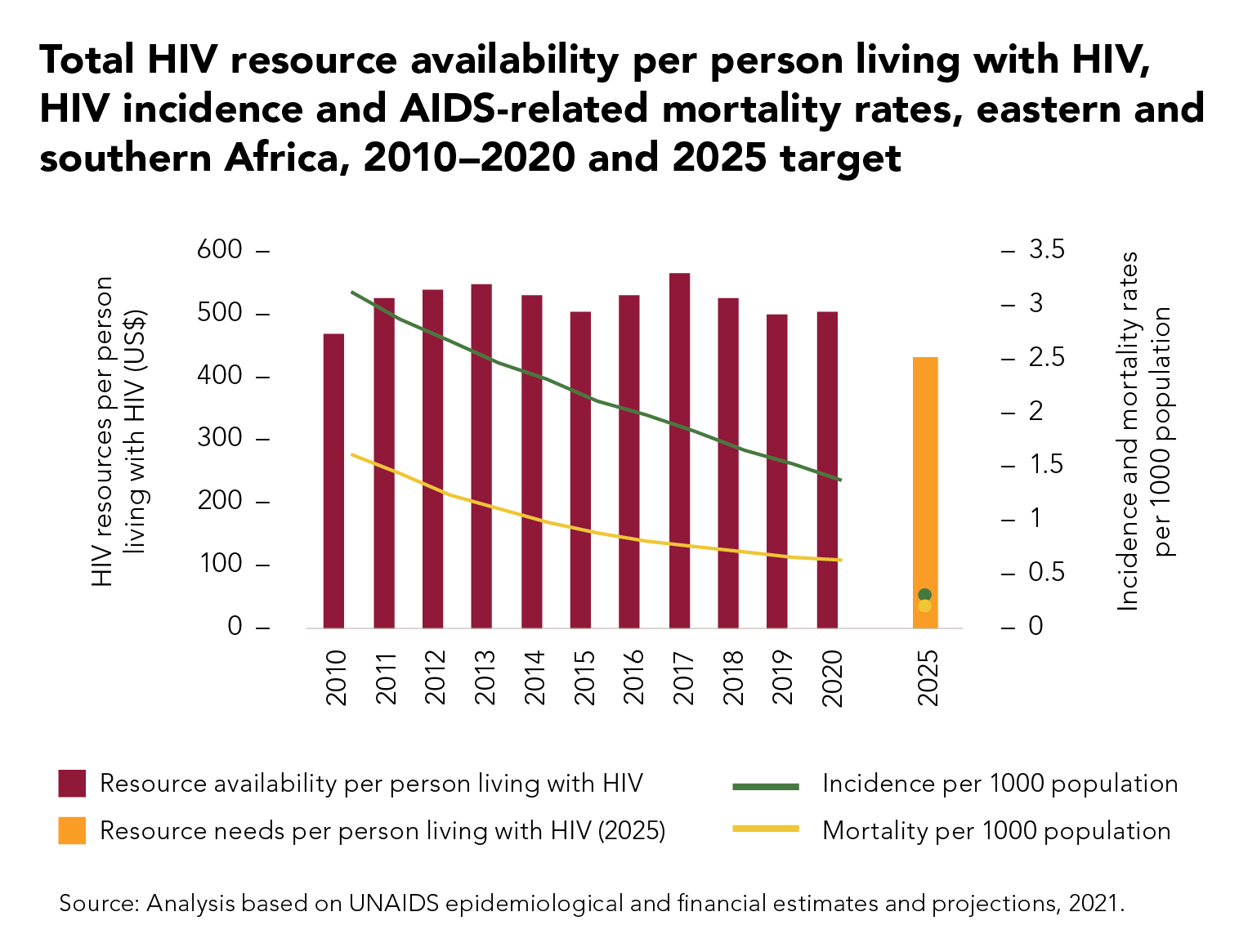
Further, the financial architecture supporting the expansion of medical interventions is under significant strain. Although incidence and mortality rates have declined, HIV resources available per person have remained uneven. Data published by UNAIDS confirm that the funding trajectories fell short of the 2025 target, creating a critical gap in the resources required to sustain regional progress (see Figure 1). This shortfall is particularly concerning because it occurs just as health systems are proving their technical capacity through high-performance metrics.
Systemic disconnect
To understand how this policy gap plays out in young people’s lives, we need to look beyond national averages. A study from Soweto offers a sobering snapshot: 23% of pregnancies among girls aged 13-16 ended in abortion, as did roughly 15% among those aged 17-19. These figures suggest that adolescent reproductive health needs are not being adequately met.
This sits uneasily alongside a more optimistic national story on HIV. By 2022, South Africa had made significant progress: among people aged 15 and older living with HIV, about 90% knew their status, 91% of those were on treatment, and nearly 94% of those on treatment were virally suppressed. This demonstrates that the health system’s clinical machinery can perform at a high level.
Yet national averages are deceptive. The same system that delivers treatment efficiently is far less effective at prevention and youth-centered care. In places like Soweto, high rates of adolescent abortion point not simply to early sexual activity but to missed opportunities for earlier engagement and support.
Evidence from Lesotho deepens this picture. Nearly 17% of women report a history of Non-Consensual First Sex (NCFS), an experience statistically associated with higher rates of high-risk behaviors and HIV infection later in life. What policy frameworks often label as “high-risk behavior”, implying individual agency, frequently reflects trauma and structural disempowerment.
Mobility adds a different kind of structural exposure. Young people who migrate for work or survival are often cut off from family support systems and excluded from health services designed for stable populations. Their vulnerability is not incidental; it is produced by the social and economic conditions they navigate.
The limitations of information and the social ecosystem
Traditional HIV prevention policy has followed a linear logic: provide risk information and behavior will change. However, operational research across six countries — Eswatini, Lesotho, Malawi, Mozambique, South Africa, and Zambia — shows a more complex reality. While knowledge is essential, it is often constrained or overridden by the social environments in which young people live.
Our findings show that interventions are most effective when they engage this broader ecosystem: peers who reinforce protective norms, teachers who create safe spaces, families who support rather than stigmatize, and community leaders who challenge harmful gender expectations. A young woman may understand HIV transmission, but if transactional sex is normalized for economic survival, or refusing an older partner risks homelessness, knowledge alone cannot shape her choices.
Even where norms begin to shift, structural barriers remain. Health education cannot translate into protective behavior when stigma, economic dependency, rigid gender hierarchies, or inflexible health systems persist. Effective prevention requires transforming the social and structural environment, not simply informing individuals.
Rigid infrastructure versus fluid lives
Perhaps the most pressing aspect of this policy challenge is that health system design often works against the very populations it seeks to serve. Research identifies restrictive laws, provider bias, and weak referral systems as major barriers, particularly for migrants and sex workers. Even well-funded programs will struggle if the legal and administrative environment remains hostile.
Service uptake depends on provider attitudes, flexibility, and alignment with social norms and mobility patterns. Young people engage when services reflect their realities: accessible hours, respectful care, and assured confidentiality. Accessibility is shaped less by location than by trust, cultural sensitivity, and responsiveness.
The evidence points to an uncomfortable conclusion: Southern Africa’s HIV response has optimized the wrong outcomes. Health systems excel at treatment but continue to fall short on prevention among those most at risk. Addressing this requires more than incremental reform. Epidemic control depends not only on clinical metrics but on structural change: legal protections for vulnerable populations, economic policies that reduce survival-driven risk, and health services aligned with young people’s lived realities.








{kind=link}